
Ongoing breakthroughs in technology have had a positive impact on many different disciplines. Recent technological developments have enabled us to leap forward in medical research and the subsequent treatment of patients. We are now able to observe activity in the brain once never imagined.
It has long been known that a person’s behavior and mental attitude can have an impact on their beliefs and what may have become habitual behavior. These habits are imprinted on the brain in the form of neural pathways. In thinking in different ways, we have the ability to create new pathways, possibly creating entirely new ways of thinking, a new belief system, and different way of operating. This is a common practice in Buddhism, where the mind is observed from a distance and positive practices are adopted in place of negative ones. We are all familiar with modern publications that encourage us to harness our thinking, and to maximize our positivity in order to manifest those things we believe will bring us happiness.
Brain researchers have long observed the activity of the brain. Members of the medical community have sought to discover which areas of the brain determine which behavior, and how this is revealed in a mental deficiency or illness, so that they can then devise an appropriate treatment. Neurophysiologists track the activity of neurons and are able to detect electrical signals in the brain. Functional imaging machines allow visibility and documentation of the brain processes. Researchers have now developed a method to harness that activity making what was once impossible, possible. Both new research in neuroscience and expansions in technology are now allowing paralyzed patients to go beyond previous limitations.
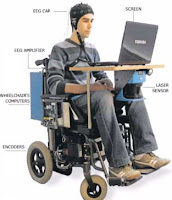
In the case of Lou Gehrig’s disease, patients “progressively lose their ability to move, speak and breathe” (Singer). However, most of them have an entirely normal thinking capacity, regardless of other obvious disabilities. Now a non-invasive EEG procedure (using electroencephalograms) allows patients to communicate. A technician does a one-time EEG cap fitting on the patient. Electrodes within the cap detect the patient’s brain activity from the surface, without having to actually penetrate the delicate organ. Various options are posed to the patient who then has the ability to make a selection simply by thinking. Electrical signals are recorded, amplified and processed by the computer. Similar systems, used with prosthetics, detect small muscle movements, but fall short when a patient loses all ability to control their muscles. It is only through findings in neuroscience that these findings have become available. Doctors are working to make a simplified in-home version of this technology available on a large scale and at a reasonable price. This advancement holds several hopeful implications, including improvements for patients in the areas of communication and mobility.
 For further reading & research:
For further reading & research:
http://www.dana.org/news/brainhealth/detail.aspx?id=10060