
Friday, August 14, 2009
2010: A Mindfulness Odyssey
In the last ten years, and beyond, there has been a steadily growing interest in the neurological benefits of practicing mindfulness as alternative to synthetic medication and existing psychoanalytical explanation for ailments like ADHD. For example, many neuroscientists have been studying the effects of meditation on patients with ADHD and find it to be a highly beneficial way of dealing with its symptoms. Meditation, in general, is a mindfulness exercise where the attention one submits is upon a very specific thing. For the meditation technique known as Vipassana, the practitioner begins with full attention on the breath advancing to full attention on the rest of the body. If done effectively, one’s attention becomes acutely aware of things happening within the body, that full observation of its processes is achieved. Susan Smalley Ph.D., a committed blogger for the Huffington Post and founder of the Mindful Awareness Research Center (MARC) at UCLA, has a vested interest in advancing the applicability of meditation as well as other mindfull practices as a solution to attention span and hyperactivity disorders. After studying autism and ADHD for 25 years, she decided upon a scientific approach different from anything she was accustomed to. Even though the medical treatment cured her of her cancer, she believed something more profound to be causing her illness. That is when she turned inward. In all her life, the pursuit of knowledge, reading books, that all she needed existed in a world governed by reason alone never allowed for importance to be given to her own intuition (the body). So she practiced meditation among other holistics, which led her to the profound realization of all things sharing interconnectivity. In her discovery, she learned of the importance of directing her attention away from external influence. There she came to distinguish between the use of reason as a foundation to support an understanding of illness and the sheer potential and efficacy of the human brain to do the same. Instead of books and logic, she turned to her breath, her body itself, to guide her. In the holistic approach, the body as a whole is observed and every part sought to equilibrate.
If the problem with attention deficit disorders is an inability to sustain attention, and meditation is the practice of sustaining attention and its benefits are scientifically measurable, it seems perfectly natural, raw if you will, to employ it. Meditation is basically an attention training program. As Dr. David Rabiner, Director of Undergraduate Studies in the Department of Psychology and Neuroscience at Duke University puts it, meditation is, “paying attention to attention.” However, its use is currently not acknowledged as a provable treatment because research has not yet been published. There is currently an abundance of research being conducted and meditation is believed to be helping with all sorts of issues like, empathy, peace and harmony, stress, insomnia and of course attention deficit.
One very basic way of thinking about how meditation can be considered a solution to ADHD is by looking at a very simple example of an attention span experiment conducted by Dr. Richard Davidson, University of Wisconsin, seen here: http://www.scientificamerican.com/video.cfm?id=1844697211. In the experiment, two groups are tested to study their ability to spot numbers within a rapidly changing series of letters. The group that meditated for three months was able to see all the numbers; the group that did not meditate missed some. This experiment illustrates the notion that a too active mind may be missing out on pertinent information.
Arguably, the prevalence of these problems in our society is a result of the structure of the modern world we are all a part of and contribute to. We are inundated by mass information and mass technologies and we need an acute attention span to run them all productively. For some this leads to mass overload and the inability to navigate in a calm efficient way.
I can relate my own experiences with attention training and the benefits observed. In the summer of 2008, I completed an intensive 10 day Vipassana meditation retreat http://www.dhamma.org/ in North Fork, CA. Among some very important precepts in place while at the retreat, students were also to commit to a vow of silence, called Noble Silence, for the entire 10 days, which meant that you were not allowed to talk under any circumstances to anyone, except of course in an emergency. It also meant that it was in one’s benefit to refrain from making eye contact with anyone. These extremes are probably impractical in our daily lives, but it was an absolutely necessary instrument for students of Vipassana so that experientially, the technique could be learned without distraction. Not talking, not paying attention to anyone but your self for hours on end, let alone days, is a significantly influential way to keeps one’s attention extremely tuned to oneself without distraction. With 10 days of silence, one has ample opportunity to reflect on the bindings, the attachments, and the vices of the external world over the mind. To quote S.N. Goenka, the major proponent for this type of meditation, Vipassana is simply a technique to end suffering (http://www.dhamma.org/en/goenka.shtml). It is the invention of Gotama, the Buddha, in India, over 2500 years ago. It is described as the Art of Living. http://www.dhamma.org/en/art.shtml. Being so acutely tuned to oneself in effect allows for new perspectives of the world. For example, paying attention only to yourself for extended periods of time, gives you the ability to assess the disciplinary nature of the mind, what objects capture attention. In practicing meditation, while attention is placed wholly on the body itself and nothing more, the practitioner is forced to his/her own awareness of attachments to external objects i.e., agitations and disharmonies perhaps related to ego, that are consequently distributed to everyone around us. An example of this would be anger felt for being cut off on the road and the consequent flipping of a bird. Other examples are jealousy, envy, pride.
Thursday, July 30, 2009
EEG & Neuroscience

Ongoing breakthroughs in technology have had a positive impact on many different disciplines. Recent technological developments have enabled us to leap forward in medical research and the subsequent treatment of patients. We are now able to observe activity in the brain once never imagined.
It has long been known that a person’s behavior and mental attitude can have an impact on their beliefs and what may have become habitual behavior. These habits are imprinted on the brain in the form of neural pathways. In thinking in different ways, we have the ability to create new pathways, possibly creating entirely new ways of thinking, a new belief system, and different way of operating. This is a common practice in Buddhism, where the mind is observed from a distance and positive practices are adopted in place of negative ones. We are all familiar with modern publications that encourage us to harness our thinking, and to maximize our positivity in order to manifest those things we believe will bring us happiness.
Brain researchers have long observed the activity of the brain. Members of the medical community have sought to discover which areas of the brain determine which behavior, and how this is revealed in a mental deficiency or illness, so that they can then devise an appropriate treatment. Neurophysiologists track the activity of neurons and are able to detect electrical signals in the brain. Functional imaging machines allow visibility and documentation of the brain processes. Researchers have now developed a method to harness that activity making what was once impossible, possible. Both new research in neuroscience and expansions in technology are now allowing paralyzed patients to go beyond previous limitations.
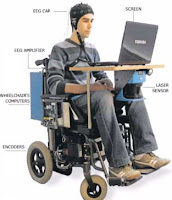
In the case of Lou Gehrig’s disease, patients “progressively lose their ability to move, speak and breathe” (Singer). However, most of them have an entirely normal thinking capacity, regardless of other obvious disabilities. Now a non-invasive EEG procedure (using electroencephalograms) allows patients to communicate. A technician does a one-time EEG cap fitting on the patient. Electrodes within the cap detect the patient’s brain activity from the surface, without having to actually penetrate the delicate organ. Various options are posed to the patient who then has the ability to make a selection simply by thinking. Electrical signals are recorded, amplified and processed by the computer. Similar systems, used with prosthetics, detect small muscle movements, but fall short when a patient loses all ability to control their muscles. It is only through findings in neuroscience that these findings have become available. Doctors are working to make a simplified in-home version of this technology available on a large scale and at a reasonable price. This advancement holds several hopeful implications, including improvements for patients in the areas of communication and mobility.
 For further reading & research:
For further reading & research:
http://www.dana.org/news/brainhealth/detail.aspx?id=10060
Neural Plasticity
We live in a world where we have the ability to experience feelings, sight, sounds and taste. Through these senses we increase the development of our brain. Our brain continuously adapts to the world around us, from the people that surround us, the experiences we face, the food we eat, and even the air we breathe. The ability of the brain to reorganize in response to its environment is called Neural Plasticity. This ability is not hard to notice, meaning everyday we can see the brain working as we learn a new skill, recall an recent event, and recover from a loss and or injury. Depending on the individual, Neural Plasticity occurs throughout development, it varies from birth through childhood and maturity. Through research it is said that neural plasticity is supported by the formation and elimination of synapses. A synapse is a small gap through which information flows from one neuron to another cell. The elimination of neurons occurs when the brain reorganizes neural connections and selective neurons which are not activity-dependant are eliminated.
Upon studying the brain of a newborn baby, scientists discovered features of early postnatal brain development the speed synapses are formed. At the age of 2 the brain of a child contains 100 trillion synapses- twice as many as in the adult brain. Early postnatal plasticity comes from studies of the primary visual cortex, whose development is shaped by visual experience during the first few months of life. The visual cortex is a region of the cerebrum that is responsible for processing visual information gathered by the eye. The early weeks and months of a baby’s life are crucial for establishing neural circuits within the visual system; other cortical functions such as touch, hearing, emotion, and memory also undergo critical periods of development. Touch is not only comforting to an infant but is vital to the formation of “touch circuits” within the developing brain. The sense of touch depends on proper wiring between touch receptors in the skin and neurons in the sensory cortex.
Learning and Memory are two of the most fundamental processes that govern our lives. Learning is the ability to acquire new knowledge through instruction or experience. Memory is the process by which knowledge is retained over time. Both are closely linked examples of neural plasticity. Songbirds learn to sing by imitation similar to the way humans learn language. Functional brain imaging studies of string instrument players have shown the cortical representation of the fingers of their left hands increases in proportion to the length of time they practice as children (5 to 20 years). The same theory applies to people blind from birth; they become functionally linked to touch stimulation of the fingers associated with Braille reading. Although scientists do not entirely understand the mechanisms for learning and memory but believe that the answers lie at the synapse that plays an important role in learning and memory.
Neural Plasticity also forms the ability to recover from brain damage caused by injury or disease. When any sort of damage is caused to the brain, the brain has many ways in replacing and or fixing itself. One of the ways the brain can compensate for a lost cause would be rerouting circuits to different regions of the brain. Another way that we can do to help repair the brain is by therapy. In some cases stroke patients who have lost the ability to speak or use a hand have been shown to regain some or most of their lost function within weeks and months. Unfortunately attempts made by the brain to compensate for the damage are not always successful or even sufficient to promote recovery of lost functions.
Nature as well as nurture influences the brain in important ways. Neural plasticity is the ability of the brain to reorganize its neural circuits in response to experience. Every day after birth to maturity we learn a new skill, memorize an experience, and adapt to a loss and injury.
For further reading refer to: Brain Development, Lakshmi Bangalore or visit
http://www.amazon.com/Brain-Development-Matter-Lakshmi-Bangalore/dp/0791089541/ref=sr_1_22?ie=UTF8&s=books&qid=1248982619&sr=8-22
Wednesday, July 29, 2009
The Phantom Limb
Phantom Limb syndrome was first acknowledged in 1552 by a French surgeon by the name of Ambroise Pare. Ambroise noticed these phenomenons with soldiers who have felt pain in their amputated limbs. Later in 1871 this disorder “Phantom Limb” was given its name by Mitchell, S. W.
The Phantom Limb syndrome is neurological disorder experienced by 50 to 80% of individuals who has previously undergone an amputated limb. This abnormal sensation can either be painful or non-painful, but the majority of the sensations experienced by individuals have been reported to be painful. Phantom sensations my also occur in other parts of the body other then the limb, such as an extraction of a tooth or a removal of an eye. The majority of people with Phantom Limb experience pain ranging from burning and shooting pain that feels like tingling of pins and needles. The remaining patients will sometimes experience the act of gesturing, itching sensations, twitches, and even try to pick up objects. In Studies by Ramachandran and Blakeslee, they describe that some patients descriptions of their limbs do not match what they’re actual limbs should be, in example, some patients would report their phantom limbs being too short. In another experiment conducted by Ramachandran and Blakeslee, a patient was ordered to grab a cup of coffee with his phantom limb, as the patient confirmed that he was reaching out, the cup was pulled away. The response received from the patient was pain even though his fingers were illusionary.
The dominant theory behind the reasoning for Phantom Limb was believed that it was associated with severed nerve endings called “neuromas”. Due to the severed nerve ending, the nerves would become inflamed, and was thought to send anomalous signals to the brain, causing abnormal interpretations by the brain as pain. Later this theory was proved as a failure as surgeons performed surgery to the amputees, hoping that shorting the stump would prevent the inflamed nerve endings, but instead the sensations heightened.
During the 1990s Tim Pons, at the National Institutes of Health, presented that the human brain can reorganize itself if sensory input were to come to a halt. With these new results, Vilayanur S. Ramachandran discovered the neuroplasticity maybe the explanation to the Phantom Limb Syndrome. Ramachandran believed that the specific explanation for this disorder was caused by map expansion neuroplasticity. Expansion neuroplasticity is the function of the brain where the local brain regions that are responsible for performing one type of function and reflected in the cerebral cortex as “maps”, can attain unused phantom maps. To further carry out his experiment, Ramachandran performed a test on an amputee by touching the side of the patients face with a cotton swab; it resulted in the patient also feeling the same sensation felt by his face was also felt by the patient’s phantom limb. Also a brain scan to the amputee using a magnetoencephalography (MEG) showed that the brain map for the patients face had taken over the adjacent area of the arm and hand brain map. With the data Ramachandran concluded that the amputated arm and hand’s brain map was starved for input therefore sending out growth-stimulating proteins that created neuronal sprouting from the face map which was stored in the adjacent are of the brain.
In some cases the symptoms of phantom limb syndrome undertakes on its own with some patients, others still experience severe symptoms, sometimes pain that cause debilitation. In this type of cases the symptoms can be suppressed through medication, hypnosis, shock therapy and acupuncture. Another alternative treatment is a novel therapy created by Ramachandran called the “Mirror Box”. It has been used by a small amount of patients, where the box mirrors the remaining limb of the patient to the missing phantom limb creating an illusion as if the missing limb is still intact. Although the success of this method is not completely understood, reports have shown that several patients have sustained long term relief.
Subscribe to:
Posts (Atom)